 |
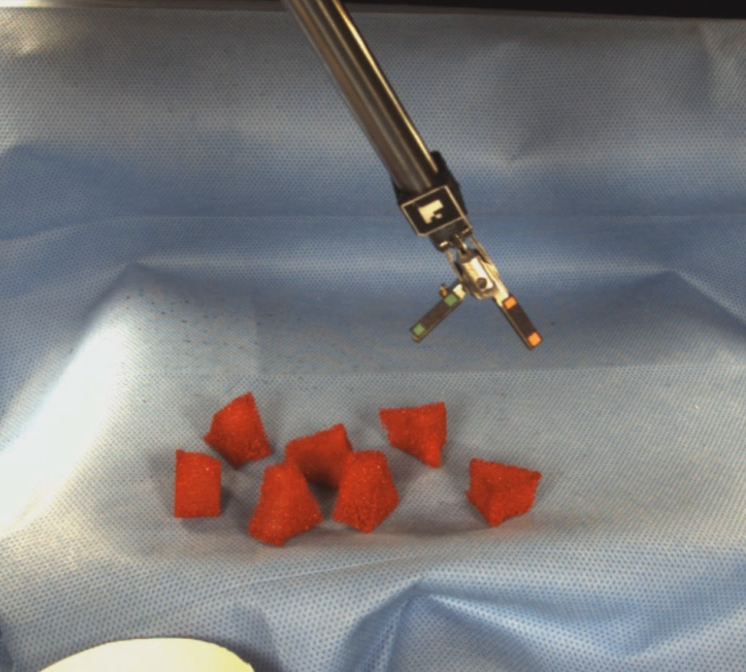 |
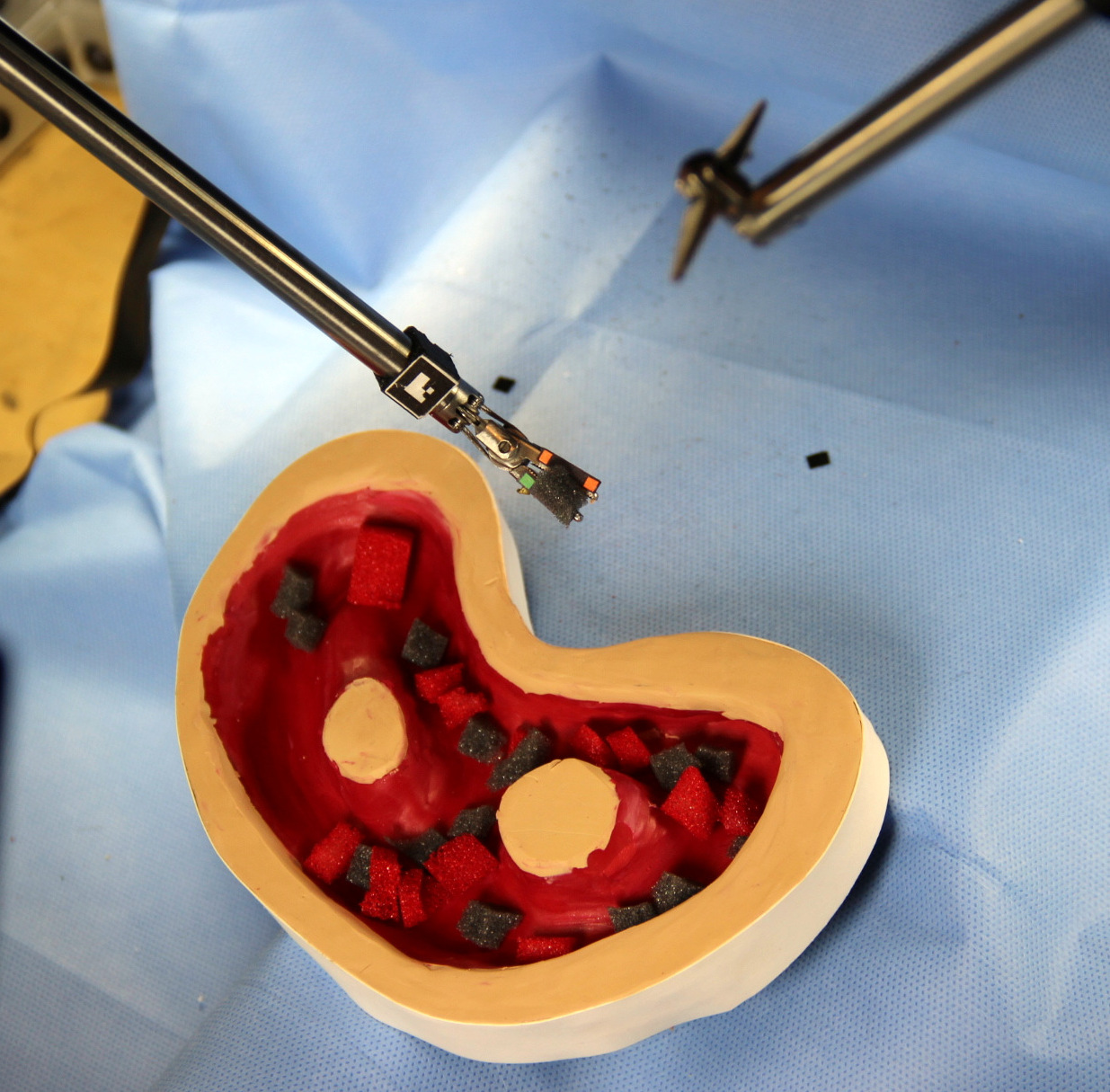
| A mock debridement setup | Another mock debridement setup |
| |
|
| A mock debridement setup | Another mock debridement setup |
A video of the Raven performing a mock debridement task on our setup.
In this paper, we introduce surgical debridement as a relevant subtask for autonomous surgical robotics. Surgical debridement 6 a tedious surgical sub-task in which dead or damaged tissue is removed from the body to allow the remaining healthy tissue to heal. Autonomous surgical debridement requires perception to locate fragments, grasp and motion planniree trajectories for one or more arms and grippers to grasp them, and control to deposit them into a receptacle. We study autonomous multilateral execution of this subtask.
Surgical debridement has several features that make it attractive for autonomous operation. It is a tedious task, which means automation could reduce surgeon fatigue. A simulation of the task can be performed with only a gripper, and it involves detection, grasping, and motion planning components.Importantly, the task or any one of its components can be approximated with varying degrees of realism, allowing autonomous surgical robots to start with simple environments and build up to more and more realistic situations.
We consider an idealized environment in which fragments designated as damaged tissue are distributed throughout the environment. The robot must find the damaged tissue fragments, grasp them, and place them in a receptacle. The level of complexity for different aspects of the task can be varied, from providing fragments to be avoided, to situating the fragments in a tissue phantom, even to attaching the fragments to the work surface and requiring a cutting action for removal. Alternatively, any or all of these may be simplified to provide a low barrier to entry for autonomous surgical robotics research.The goal is to facilitate safe (collision-free) multilateral autonomous execution of the surgical debridement task using a surgical robot.
Our experiments with autonomously sensing, grasping, and removing over 100 fragments suggest that it is possible for an autonomous surgical robot to achieve robustness comparable to human levels for a surgically-relevant task, although for our current implementation, execution time is 2-3 times slower than human levels. Both autonomous and teleoperated system were able to successfully complete all trials, recovering from both grasp and motion failure modes. The grasp failure rate was slightly higher for teleoperation than for the autonomous system. The slower execution of the autonomous system was primarily due to planning and perception; the total amount of time spent in motion for two-arm autonomous operation was slightly less than the total time for teleoperation. This suggests that optimized perception implementations and improved state estimation (which would reduce the need for costly replanning) could significantly reduce overall execution time.
| Human | Autonomous | ||
| Local Teleoperation | 1 arm | 2 arm | |
| Total number of fragments | 30 | 60 | 60 |
| Avg. time per fragment (s) | 29.0 | 91.8 | 60.3 |
| Avg. time for perception (%) | -- | 12.1 | 10.0 |
| Avg. time for planning (%) | -- | 32.8 | 36.6 |
| Avg. time for arm movement (%) | -- | 55.1 | 45.7 |
| Avg. time waiting on other arm (%) | -- | -- | 7.7 |
| Avg. number of replanning steps | -- | 11.06 | 10.58 |
| Fragment false negative (%) | 0.0 | 1.9 | 0.0 |
| Fragment false positive (%) | 0.0 | 0.0 | 0.0 |
| Pickup false negative (%) | 0.0 | 0.0 | 0.0 |
| Pickup false positive (%) | 0.0 | 0.0 | 3.6 |
| Grasp failure (%) | 5.0 | 3.5 | 3.6 |
| Grasp multiple fragments (%) | 0.0 | 5.2 | 7.1 |
| Pickup failure (%) | 0.0 | 0.0 | 0.0 |
| Drop en route (%) | 0.0 | 0.0 | 1.8 |
| Dropoff failure (%) | 0.0 | 0.0 | 0.0 |